How to Read SIBO Test Results and Next Steps

If your SIBO breath test came back negative but you're still experiencing digestive symptoms, you're not alone—false negatives can arise when the carbohydrate substrate fails to reach the small intestine due to an underlying process.
Key Takeaways
SIBO breath test results show positive when hydrogen rises ≥20 ppm within 90 minutes or methane reaches ≥10 ppm at any time during testing, though interpretation guidelines may vary among practitioners
False negatives can occur in 20-30% of cases due to hydrogen sulfide-producing bacteria, slow transit, or improper test preparation
Positive results typically require antimicrobial treatment like rifaximin or herbal protocols, while negative results may need alternative testing methods
Test accuracy depends heavily on proper preparation including 12-hour fasting, avoiding antibiotics for 2-4 weeks, and following specific dietary restrictions
Understanding SIBO breath test results can feel overwhelming when the numbers don't match expectations or symptoms persist despite negative findings. The complexity of interpreting hydrogen and methane measurements, combined with the test's inherent limitations, means many patients need guidance beyond the basic positive or negative designation.
Your SIBO Breath Test Results: What Those Numbers Actually Mean
SIBO breath test results measure gas production from bacterial fermentation in the digestive tract. The test tracks hydrogen and methane levels in exhaled breath after consuming a sugar solution, typically glucose or lactulose. These gases indicate bacterial activity that shouldn't occur in the small intestine under normal circumstances.
Normal baseline readings should remain below 16 parts per million (ppm) for hydrogen before starting the test. Higher baseline levels often signal improper preparation or existing bacterial overgrowth. The timing and pattern of gas elevation throughout the testing period provides crucial diagnostic information about bacterial location and activity levels.
Healthcare providers analyze both the magnitude of gas increases and when they occur during the testing window. Dr. Derek Cook at Healthflow Naturopathic emphasizes that proper interpretation requires understanding these patterns alongside clinical symptoms rather than relying solely on numerical thresholds.
Understanding Hydrogen vs. Methane Measurements
Hydrogen elevation thresholds: ≥20 ppm rise within 90 minutes (North American Consensus) or ≥12 ppm for glucose protocols
Hydrogen gas elevation indicates bacterial fermentation of the test substrate within the small intestine. The North American Consensus guidelines establish a 20 ppm rise above baseline within 90 minutes as the diagnostic threshold for SIBO. However, glucose breath tests may use a lower threshold of 12 ppm due to glucose's rapid absorption properties.
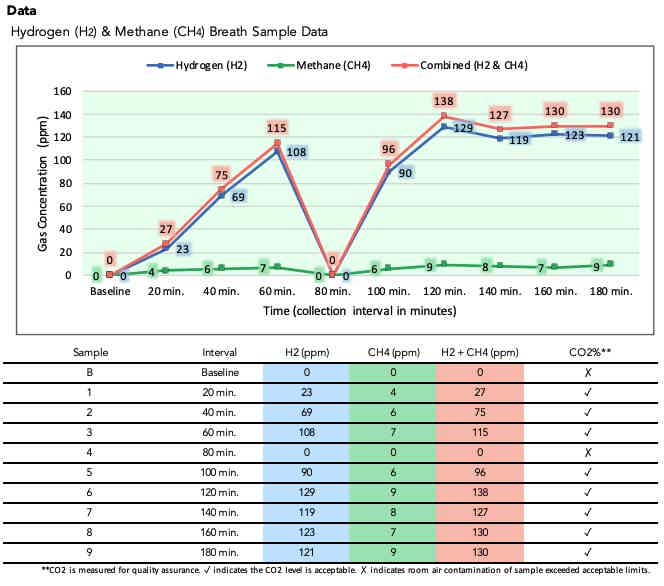
The 90-minute timeframe corresponds to normal small intestinal transit time. Gas production within this window suggests bacteria are fermenting the test sugar before it reaches the colon, where bacterial fermentation naturally occurs. Peak hydrogen levels typically occur between 60-90 minutes in positive SIBO cases.
Methane patterns: ≥10 ppm at any time indicates Intestinal Methanogen Overgrowth (IMO)
Methane production differs significantly from hydrogen, requiring only 10 ppm elevation at any point during testing to indicate Intestinal Methanogen Overgrowth (IMO). Methane-producing organisms called methanogens create this gas through a different metabolic pathway than hydrogen-producing bacteria. IMO represents the updated terminology for methane-dominant SIBO, as methanogens are archaea rather than bacteria.
IMO often correlates with constipation-predominant symptoms because methane slows intestinal motility. Unlike hydrogen, methane levels may remain elevated throughout the entire testing period rather than showing distinct peaks. Some patients produce both hydrogen and methane, creating mixed patterns that require careful interpretation.
When Your Test Results Show SIBO Positive
Early peak patterns (within 90 minutes): Proximal small intestine bacterial overgrowth
Early gas elevation within the first 90 minutes indicates bacterial overgrowth in the proximal (upper) small intestine. This pattern typically shows sharp increases in hydrogen or methane levels shortly after consuming the test substrate, often peaking between 60-90 minutes.
Proximal SIBO frequently causes symptoms like bloating, nausea, and upper abdominal discomfort shortly after eating. The bacterial overgrowth occurs close to the stomach, leading to rapid fermentation of consumed carbohydrates and sugars before proper digestion can occur.
Late rise patterns (after 2 hours): Distal overgrowth or rapid gastrointestinal transit
Gas elevation occurring after the 2-hour mark suggests either distal (lower) small intestine overgrowth or unusually rapid gastrointestinal transit. Rapid transit can cause the test substrate to reach colonic bacteria sooner than expected, creating late-positive results that may not represent true SIBO.
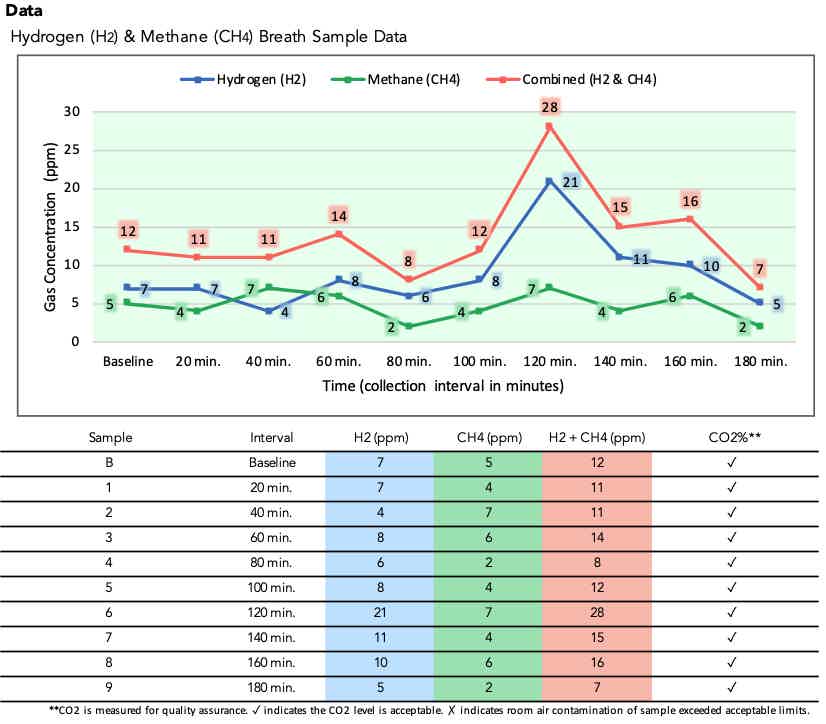
Distinguishing between distal SIBO and rapid transit requires clinical correlation with symptoms and medical history. Patients with rapid transit often experience diarrhea-predominant symptoms, while true distal SIBO may present with more varied digestive complaints affecting the lower abdomen.
Mixed gas elevation scenarios and interpretation challenges
Some patients produce both hydrogen and methane during testing, creating complex interpretation scenarios. Mixed patterns may show hydrogen peaks early with sustained methane elevation, or alternating elevations of both gases throughout the testing period.
These mixed patterns often indicate diverse bacterial populations within the small intestine. Treatment approaches may need to target both hydrogen and methane-producing organisms, requiring combination antimicrobial protocols rather than single-agent therapy.
Negative Results Don't Always Mean No SIBO
False negative factors: Slow transit time, improper preparation, and substrate choice
False negative results occur in 20-30% of SIBO cases due to various factors affecting test accuracy. Slow gastrointestinal transit can delay substrate delivery to bacterial populations, causing gas elevation beyond the diagnostic window. Poor test preparation, including inadequate fasting or recent antibiotic use, significantly impacts bacterial populations and gas production.
Substrate choice also influences detection rates. Lactulose testing may detect SIBO throughout the entire small intestine but can cause false positives due to rapid transit. Glucose testing offers higher specificity but may miss distal small bowel overgrowth since glucose absorbs quickly in the proximal intestine.
Hydrogen sulfide-producing bacteria: When very low hydrogen/methane suggests H2S SIBO requiring specialized testing
Hydrogen sulfide-producing bacteria consume hydrogen gas during metabolism, creating falsely low hydrogen readings despite active bacterial overgrowth. These bacteria produce hydrogen sulfide (H2S), which isn't measured by standard breath testing equipment.
H2S SIBO often presents with particularly severe symptoms including sulfurous belching, intense bloating, and digestive distress. Patients may have strong clinical suspicion for SIBO with normal or low breath test readings. Specialized H2S breath testing or alternative diagnostic methods become necessary for accurate diagnosis.
Test Preparation Issues That Invalidate Results
High baseline readings from improper fasting, poor oral hygiene, or foregut dysmotility

Elevated baseline hydrogen or methane levels above 16 ppm before substrate consumption indicate test preparation problems. Improper fasting allows residual food fermentation, while poor oral hygiene enables bacterial gas production in the mouth. Foregut dysmotility conditions like gastroparesis can trap fermentable substrates, creating elevated baseline readings.
High baseline levels typically require test postponement and stricter preparation protocols. Patients must repeat the 12-hour fasting period and may need additional oral hygiene measures or prokinetic medications to normalize baseline readings before retesting.
Medication interference and timing considerations
Several medication classes interfere with breath test accuracy. Antibiotics alter gut bacterial populations for weeks after discontinuation, requiring a minimum 2-4 week washout period. Prokinetic agents, laxatives, and antacids affect gastrointestinal transit and pH, potentially masking or exaggerating bacterial gas production.
Timing medication discontinuation requires careful coordination with healthcare providers, especially for essential medications. Some patients may need alternative diagnostic approaches if critical medications cannot be safely discontinued for adequate washout periods.
Your Next Steps Based on Test Results
Positive results: Low FODMAP diet, probiotics, rifaximin, or herbal antimicrobials
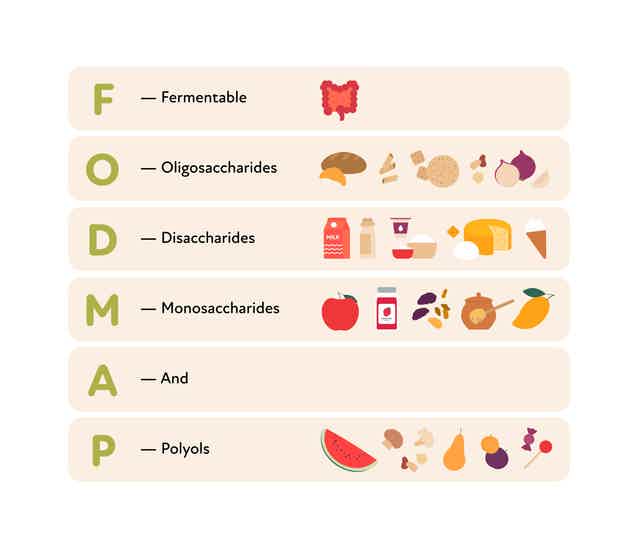
Positive SIBO breath tests typically warrant antimicrobial treatment combined with dietary modifications. Rifaximin, a non-absorbed antibiotic, represents first-line pharmaceutical therapy with proven efficacy for hydrogen-producing SIBO. Herbal antimicrobial protocols using compounds like berberine, oregano oil, and allicin offer alternative treatment options.
Low FODMAP dietary restriction helps reduce bacterial substrate availability during treatment. Selective probiotic strains, particularly Saccharomyces boulardii, may support treatment outcomes without worsening bacterial overgrowth. Treatment duration typically ranges from 10-14 days for pharmaceutical options or 4-8 weeks for herbal protocols. For a full breakdown, see how to treat SIBO naturally with a timeline.
Negative results: Alternative SIBO testing (stool, serum antibodies) and dysbiosis evaluation
Negative breath test results with persistent symptoms warrant alternative diagnostic approaches. Stool analysis can identify bacterial imbalances, inflammatory markers, and digestive function parameters that standard breath testing misses. Serum antibody testing for specific bacterial toxins may reveal immune responses to bacterial overgrowth.
Small bowel aspiration and culture remain the gold standard for SIBO diagnosis but require invasive endoscopic procedures. These tests become relevant when clinical suspicion remains high despite negative breath testing, particularly in patients with severe or refractory symptoms.
Inconclusive results: Retesting protocols due to false negative potential
Inconclusive or borderline results often require repeat testing with modified protocols. Alternative substrates, extended testing periods, or different preparation protocols may improve diagnostic accuracy. Some patients benefit from both glucose and lactulose testing to capture different aspects of bacterial overgrowth.
Clinical correlation remains vital for interpreting inconclusive results. Symptom severity, treatment response, and alternative test findings help guide therapeutic decisions when breath test results remain ambiguous.
Partner with Healthflow Naturopathic for Evidence-Based SIBO Management
Interpreting SIBO breath test results requires experience in understanding complex gas patterns, recognizing false negatives, and developing treatment strategies. The interplay between test timing, bacterial types, and individual patient factors creates unique diagnostic challenges that benefit from experienced clinical guidance.
Successful SIBO management extends beyond initial test interpretation to include treatment monitoring, dietary optimization, and addressing underlying predisposing factors. The complexity of bacterial overgrowth syndromes often requires multiple therapeutic approaches and ongoing clinical supervision to achieve lasting symptom resolution.
For SIBO testing interpretation and evidence-based treatment protocols, Dr. Derek Cook of Healthflow Naturopathic provides naturopathic care focused on digestive health optimization.
Ready to get started?
Book your free discovery call with a Naturopathic Doctor of your choice.
Free Discovery CallDisclaimer: The information in this blog is for educational purposes only and does not replace professional medical advice. Always consult a qualified healthcare provider with questions regarding your health.